What is Lordosis?
A normal spine, when viewed from behind, appears straight. From the side, the spine normally curves at the neck, the torso and the lower back area.
Lordosis is the inward curvature of a portion of the lumbar (lower back) and cervical (upper back) spine. These normal “lordotic curves” of the spine (secondary curvatures) are caused by differences in thickness between the front and back part of the discs between each vertebra (back bone) in the spine. These curves position the head over the pelvis naturally and also act as shock absorbers distributing the stress that occurs during movement.
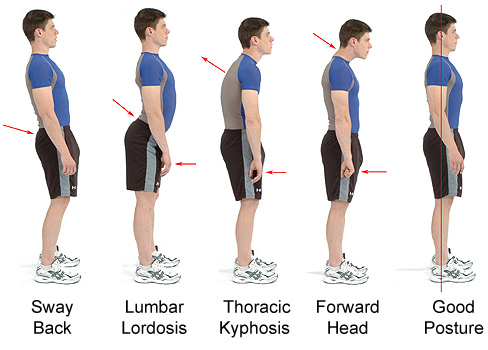
Hyperlordosis (Swayback, Saddleback, Hollow back, Anterior Pelvic Tilt)
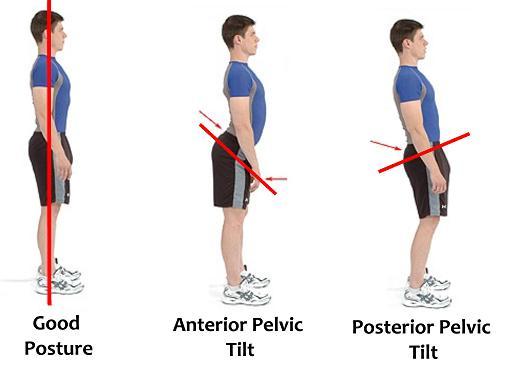
Normal spinal contours are essential for the correct movement and function of the spine. In a spine affected by hyperlordosis or an excessive or exaggerated inward curve, the vertebrae of the lumbar area are more curved, giving a swayback appearance. Excessive or hyperlordosis is commonly referred to as hollow back, sway back or saddle back, a term that originates from the similar condition that arises in some horses. A major contributing factor of lumbar lordosis is anterior pelvic tilt, when the pelvis tilts forward when resting on top of the femurs (thigh bones).
When lying on your back on a hard surface, a large degree of lordosis will appear as a space beneath the lower back and the surface. Excessive lordosis may also increase at puberty, sometimes not becoming evident until your early or mid 20s.
Hypolordosis (Flatback)
More common than hyperlordosis, Hypolordosis means there’s less of a curve in the lower back or a flattening of the lower back. This occurs because the vertebrae are oriented toward the back of the spine, stretching the disc towards the back and compressing it in the front . This can cause a narrowing of the opening for the nerves, potentially pinching them.
Lordosis Symptoms
Hyper (too much) or Hypo (too little) lordosis can cause moderate to severe lower back pain and can cause pain that affects movement. If the curve is flexible (reverses itself when the person bends forward), there is little need for concern. If the curve does not change when the person bends forward, the lordosis is fixed or locked and treatment is needed.
Causes of Lordosis
Causes of Hyperlordosis
Hyperlordosis affects people of all ages. It is common in dancers gymnasts and certain conditions can contribute to lordosis, including achondroplasia, discitis, kyphosis, obesity, osteoporosis and spondylolisthesis. Imbalances in muscle strength and length are also a cause, such as weak hamstrings, or tight hip flexors. Rickets, a vitamin D deficiency in children, can also cause lumbar lordosis. Common causes of hyperlordosis include tight lower back muscles, excessive visceral fat (belly fat), and pregnancy. Excess belly fat pulls the pelvis to the front and makes the pelvis tilt.
Causes of Hypolordosis
Hypolordosis can be congenital, acquired from sitting with bad posture, or from trauma. A common cause is whiplash trauma to the cervical spine. Hypolordosis is commonly found in teenagers with scoliosis.
Lordosis Diagnosis
To diagnose lordosis the patient’s medical history & a physical examination are necessary to determine:
- When did the excessive or diminished curve become noticeable?
- Is it getting worse?
- Does the size of the curve seem to change?
The patient is asked to bend forward and to the side to see whether the curve is flexible or fixed, how much range of motion the patient has and if the spine is aligned properly. The doctor may feel the spine to check for abnormalities. X-rays may be taken of the whole and the lower back.
A neurological assessment may be necessary if the person is having:
- Pain
- Tingling
- Numbness
- Muscle spasms or weakness
- Sensations in the arms or legs
- Changes in bowel or bladder control
How to Fix Lumbar Lordosis
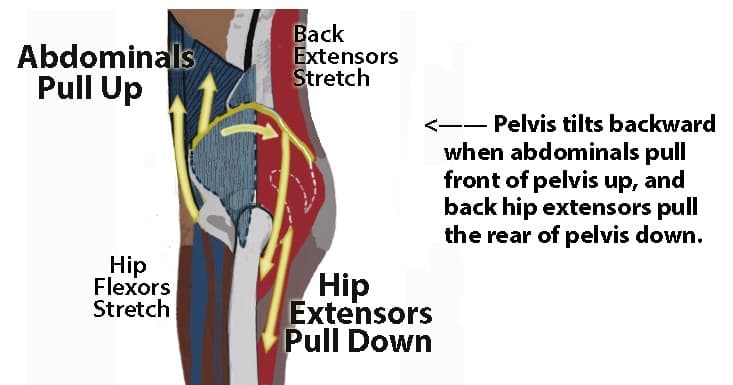
Lordosis treatment involves building strength and flexibility to increase range of motion. Lumbar lordosis treatment consists of strengthening the hip extensors (group of muscles that extend the thigh) on the back of the thighs and stretching the hip flexors (group of muscles that flex the thigh) on the front of the thighs. The muscles on the front and on the back of the thighs can rotate the pelvis forward or backward while in a standing position. They can release the force on the ground through the legs and feet.
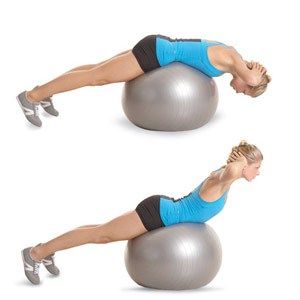
Back extensions on a exercise ball will strengthen the entire posterior chain (group of muscles on the back of the body) and help lordosis. Stiff legged deadlifts and supine hip lifts and other similar movement strengthen the posterior chain without involving the hip flexors on the front of the thighs. Neuromuscular re-education techniques are used to specifically target the problem.




Hypolordosis tends to co-occur with scoliosis. That may be due to instability in the spine caused by a lack of the normal curve. Part of scoliosis care must be to protect and strengthen the normal spinal contours. A downside of poor quality scoliosis braces and scoliosis surgery is that they both exacerbate hypolordosis in both the neck and back which weakens the spine.
If the hyperlordosis is the result of excess belly fat weight loss may be required to reverse the curve.
Hypolordosis can be corrected non-surgically through rehabilitation exercises and if done correctly, symptoms can be reduced in 3-6 months.
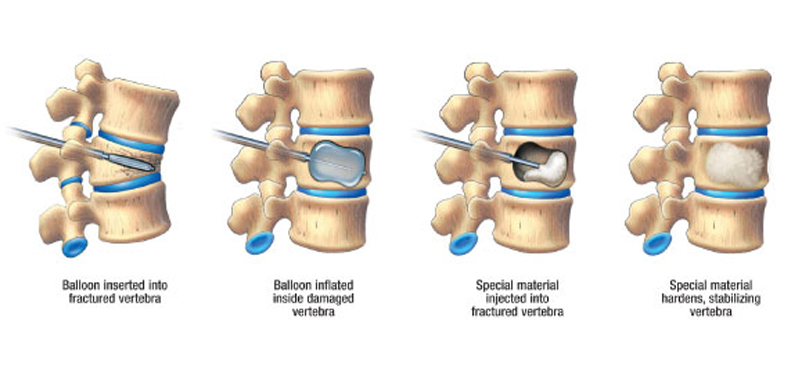
Only the most severe cases of lordosis require surgery: spinal instrumentation, artificial disc replacement and(a type of minimally invasive surgery that restores the vertebral height after a spinal compression fracture has occurred).
As with AIS, early detection is key to treating lumbar lordosis. For more information contact our office.

